Glioblastoma
- Lasya Kambhampati
- Oct 30, 2020
- 4 min read

Men are more likely to get glioblastomas than women. Age is another risk factor - the older you are, the higher risk you have. In addition, previous radiation exposure is another risk factor (this often applies to patients who have had other cancers). Race is another risk factor. Caucasian people had higher incidence rates of glioblastoma than nearly every other race. Hispanic people had the lowest rates.

Glioblastomas are malignant gliomas. A glioma is simply a tumor in the nervous system. They develop from glial cells (specifically astrocytes). Glial cells are essential for protecting neurons and keeping the brain “clean”. Each type of cell has a specific function; for example, oligodendrocytes insulate neurons. Learn more about glial cells function within the brain here. This cancer is always classified as a grade IV tumor as it is extremely aggressive and spreads rapidly. The cause of glioblastomas is not clear. However, it is known that they can develop from astrocytomas, lower-grade cancer. It is not known what causes the somewhat benign tumors to become malignant.
The tumors are often found in the frontal or temporal lobes of the brain or more generally in the cerebrum. As a result, the first symptoms are often related to issues with speech, memory, and senses. See more about the functions of these structures here. From these areas, the tumor can spread anywhere in the nervous system, including the spinal cord.

Symptoms
There are a variety of symptoms and each patient has different experiences.
Constant headaches
Seizures
Vomiting
Trouble thinking
Changes in personality
Vision issues
Trouble speaking
Risk Groups:
Numerous drugs are being developed every year to help people with glioblastomas. Normally, the drugs will focus on the distinctions between cancer cells and regular cells in order to kill specific cells. For example, ve had other cancers). Race is another risk factor. Caucasian people had higher incidence rates of glioblastoma than nearly every other race. Hispanic people had the lowest rates.
Diagnosis:
There are numerous ways to diagnose glioblastomas.
Your doctor could do a neurological exam. The exam will check your senses (i.e. hearing, vision, smell), reflexes, strength, and balance. The results of this exam in conjunction with your symptoms will help the doctor determine if your brain has been affected by a tumor.

If a tumor is suspected, an imaging test will probably be ordered. Usually, this requires an MRI or fMRI but CT and PET scans may be used as well. This will help determine the size, shape, and location of the tumor.
This therapy uses an electrical field to prevent the tumor from multiplying. Similar to an AED, TTF requires the application of pads that can transmit electrical current to your skin. e cancerous cells and how to grade them (see above for grading scale). It will also help guide treatment options.
Treatment:
The average life span after being diagnosed is 15 months. However, research and new treatments are extending that time every day. Because glioblastomas are so aggressive, it is really difficult to treat them. They are often resistant to conventional methods of therapy, requiring multiple therapies combined to see a difference. Also, the brain is limited in its ability to repair itself. The blood-brain barrier (see more here) prevents most medications from actually reaching the brain.
Surgery:
A neurosurgeon can try to remove the glioblastoma through invasive surgery. Although the goal is to remove all cancerous tissues, a complete removal is almost impossible. There are always microscopic “arms” that remain in the brain. Unfortunately, these tendrils can not be seen on our scans, and therefore, it is extremely hard to remove every single cancerous cell. Even after undergoing surgery, there is a chance that some cells will remain and cause a resurgence of the cancer. Undergoing a gross total resection, which removes over 98% of the tumor, increases the chance of remission.
Radiation Therapy:
Although this may seem counter-intuitive, considering that radiation is a risk factor for glioblastomas, radiation therapy is effective in killing cancer cells. Specifically, doctors use high energy beams such as X-rays and photons to kill the cells at specific places in your brain. It is often used after surgery to ensure that patients don’t experience reoccurrence or as a primary treatment when surgery is not possible.
Chemotherapy:

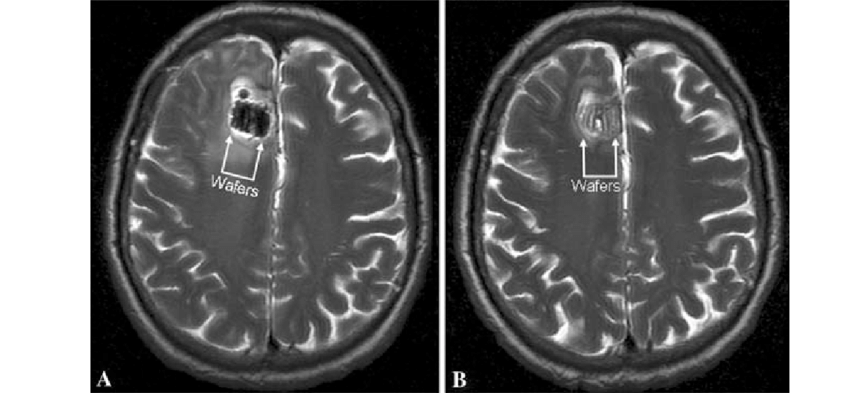


Chemotherapy, which is well known as a cancer treatment, is often used in combination with radiation therapy to treat glioblastomas. One treatment involves placing thin wafers which contain the medicine in chemotherapy in your brain during surgery (see image for more details). The wafers will slowly dissolve, killing the cells around it. This helps ensure cancer doesn’t come back. Traditional chemotherapy, which can be administered intravenously or through a pill, is also used in glioblastomas.
Tumor treating fields (TTF) therapy:
This therapy uses an electrical field to prevent the tumor from multiplying. Similar to an AED, TTF requires application of pads that can transmit electrical current to your skin.
Medications:
There are numerous drugs that are being developed every year to help people with glioblastomas. Normally, the drugs will focus on the distinctions between cancer cells and regular cells in order to kill specific cells. For example, Bevacizumab (also known as Avastin) targets the signals that cancer cells send that cause new blood vessels to form. This prevents the tumor from accessing nutrients and should lead to their death.
Resources:
- Lasya Kambhampati



Comments